
Search
- Page Path
- HOME > Search
Review Articles
- Thyroid
- T4+T3 Combination Therapy: An Unsolved Problem of Increasing Magnitude and Complexity
- Wilmar M. Wiersinga
- Endocrinol Metab. 2021;36(5):938-951. Published online September 30, 2021
- DOI: https://doi.org/10.3803/EnM.2021.501
- 9,048 View
- 336 Download
- 11 Web of Science
- 9 Crossref
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader  ePub
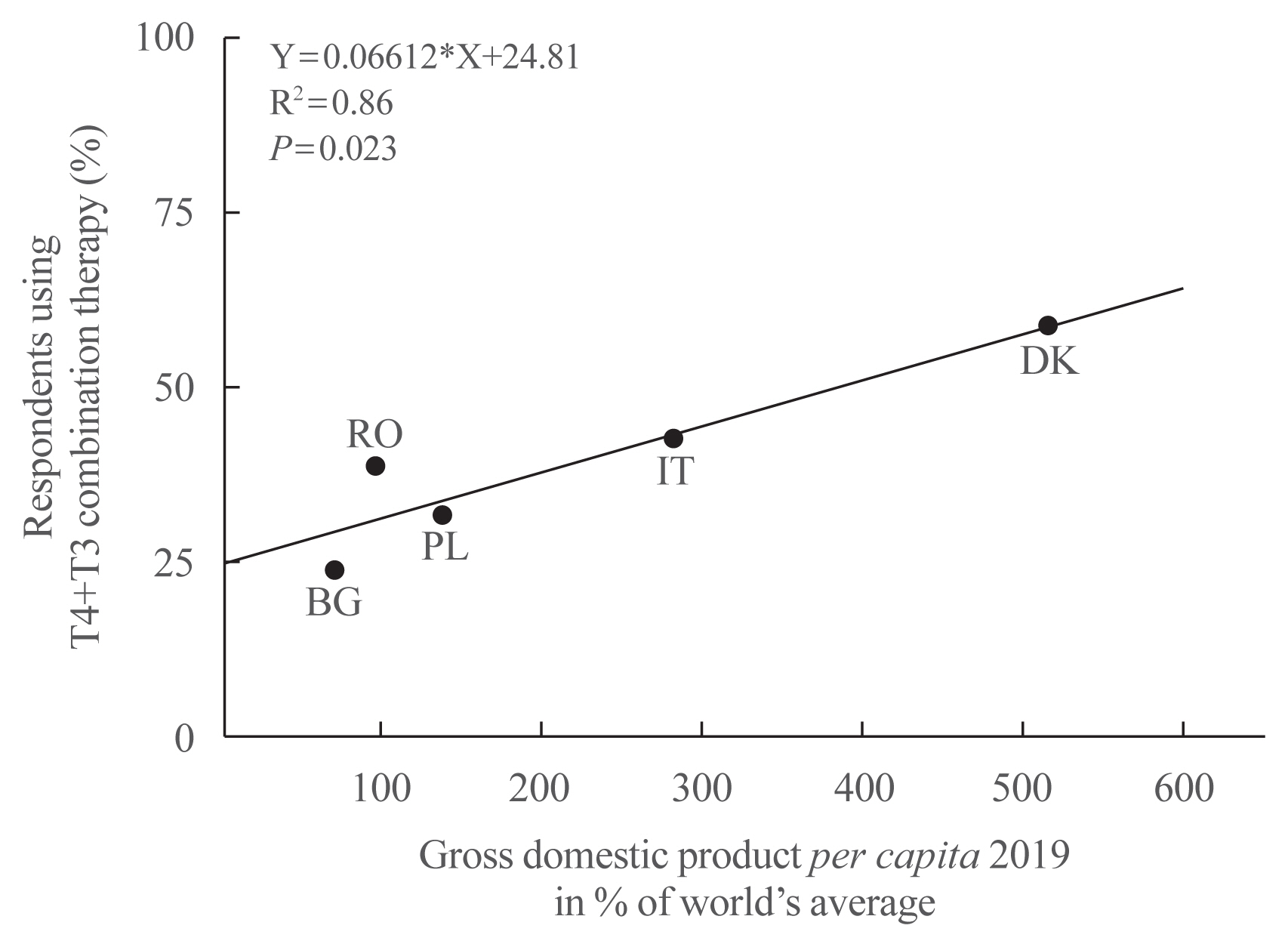
ePub - Thyroxine (T4)+triiodothyronine (T3) combination therapy can be considered in case of persistent symptoms despite normal serum thyroid stimulating hormone in levothyroxine (LT4)-treated hypothyroid patients. Combination therapy has gained popularity in the last two decades, especially in countries with a relatively high gross domestic product. The prevalence of persistent symptoms has also increased; most frequent are complaints about energy levels and fatigue (80% to 90%), weight management (70% to 75%), memory (60% to 80%), and mood (40% to 50%). Pathophysiological explanations for persistent problems are unrealistic patient expectations, comorbidities, somatic symptoms, related disorders (Diagnostic and Statistical Manual of Mental Disorders [DSM-5]), autoimmune neuroinflammation, and low tissue T3. There is fair circumstantial evidence for the latter cause (tissue and specifically brain T3 content is normalized by T4+T3, not by T4 alone), but the other causes are viewed as more relevant in current practice. This might be related to the ‘hype’ that has emerged surrounding T4+T3 therapy. Although more and better-designed trials are needed to validate the efficacy of T4+T3 combination, the management of persistent symptoms should also be directed towards alternative causes. Improving the doctor-patient relationship and including more and better information is crucial. For example, dissatisfaction with the outcomes of T4 treatment for subclinical hypothyroidism can be anticipated as recent trials have demonstrated that LT4 is hardly effective in improving symptoms associated with subclinical hypothyroidism.
-
Citations
Citations to this article as recorded by
- Association of DIO2 and MCT10 Polymorphisms With Persistent Symptoms in LT4-Treated Patients in the UK Biobank
Christian Zinck Jensen, Jonas Lynggaard Isaksen, Gustav Ahlberg, Morten Salling Olesen, Birte Nygaard, Christina Ellervik, Jørgen Kim Kanters
The Journal of Clinical Endocrinology & Metabolism.2024; 109(2): e613. CrossRef - Quality of life, daily functioning, and symptoms in hypothyroid patients on thyroid replacement therapy: A Dutch survey
Ellen Molewijk, Eric Fliers, Koen Dreijerink, Ad van Dooren, Rob Heerdink
Journal of Clinical & Translational Endocrinology.2024; 35: 100330. CrossRef - Use of thyroid hormones in hypothyroid and euthyroid patients: A survey of members of the Endocrine Society of Australia
Nicole Lafontaine, Suzanne J. Brown, Petros Perros, Enrico Papini, Endre V. Nagy, Roberto Attanasio, Laszlo Hegedüs, John P. Walsh
Clinical Endocrinology.2024; 100(5): 477. CrossRef - Use of Thyroid Hormones in Hypothyroid and Euthyroid Patients: A THESIS questionnaire survey of members of the Irish Endocrine Society
Mohamad Mustafa, Elsheikh Ali, Anne McGowan, Laura McCabe, Laszlo Hegedüs, Roberto Attanasio, Endre V. Nagy, Enrico Papini, Petros Perros, Carla Moran
Irish Journal of Medical Science (1971 -).2023; 192(5): 2179. CrossRef - Levothyroxine: Conventional and Novel Drug Delivery Formulations
Hanqing Liu, Wei Li, Wen Zhang, Shengrong Sun, Chuang Chen
Endocrine Reviews.2023; 44(3): 393. CrossRef - Re: “Exploring the Genetic Link Between Thyroid Dysfunction and Common Psychiatric Disorders: A Specific Hormonal or a General Autoimmune Comorbidity” by Soheili-Nezhad et al.
Christiaan F. Mooij, A.S. Paul van Trotsenburg
Thyroid®.2023; 33(8): 999. CrossRef - Circulating thyroid hormones and clinical parameters of heart failure in men
Iva Turić, Ivan Velat, Željko Bušić, Viktor Čulić
Scientific Reports.2023;[Epub] CrossRef - Evaluation of cortical and trabecular bone structure of the mandible in patients using L-Thyroxine
Melike Gulec, Melek Tassoker, Mediha Erturk
BMC Oral Health.2023;[Epub] CrossRef - The Impact of Hypothyroidism on Satisfaction with Care and Treatment and Everyday Living: Results from E-Mode Patient Self-Assessment of Thyroid Therapy, a Cross-Sectional, International Online Patient Survey
Petros Perros, Laszlo Hegedüs, Endre Vezekenyi Nagy, Enrico Papini, Harriet Alexandra Hay, Juan Abad-Madroñero, Amy Johanna Tallett, Megan Bilas, Peter Lakwijk, Alan J. Poots
Thyroid.2022;[Epub] CrossRef
- Association of DIO2 and MCT10 Polymorphisms With Persistent Symptoms in LT4-Treated Patients in the UK Biobank

- Thyroid
- Graves' Disease: Can It Be Cured?
- Wilmar M. Wiersinga
- Endocrinol Metab. 2019;34(1):29-38. Published online March 21, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.1.29
- 16,281 View
- 511 Download
- 44 Web of Science
- 46 Crossref
-
Abstract
PDFPubReader ePub
Whether or not Graves' hyperthyroidism can be really cured, depends on the definition of “cure.” If eradication of thyroid hormone excess suffices for the label “cure,” then all patients can be cured because total thyroidectomy or high doses of 131I will abolish hyperthyroidism albeit at the expense of creating another disease (hypothyroidism) requiring lifelong medication with levothyroxine. I would not call this a “cure,” which I would like to define as a state with stable thyroid stimulating hormone (TSH), free thyroxine, and triiodothyronine serum concentrations in the normal range in the absence of any thyroid medication. Surgery and radioiodine are unlikely to result in so-defined cures, as their preferable aim as stated in guidelines is to cause permanent hypothyroidism. Discontinuation of antithyroid drugs is followed by 50% recurrences within 4 years; before starting therapy the risk of recurrences can be estimated with the Graves' Recurrent Events After Therapy (GREAT) score. At 20-year follow-up about 62% had developed recurrent hyperthyroidism, 8% had subclinical hypothyroidism, and 3% overt hypothyroidism related to TSH receptor blocking antibodies and thyroid peroxidase antibodies. Only 27% was in remission, and might be considered cured. If the definition of “cure” would also include the disappearance of thyroid antibodies in serum, the proportion of cured patients would become even lower.
-
Citations
Citations to this article as recorded by- Multifunctional nanoparticle-mediated combining therapy for human diseases
Xiaotong Li, Xiuju Peng, Makhloufi Zoulikha, George Frimpong Boafo, Kosheli Thapa Magar, Yanmin Ju, Wei He
Signal Transduction and Targeted Therapy.2024;[Epub] CrossRef - Prenatal double-hit with aluminium and cadmium mediate testicular atrophy and hypothalamic hypoplasia: the role of oxido-nitrergic stress and endocrine perturbations
Emmanuel Okhue, Helen Ejiro Kadiri, Patrick Chukwuyenum Ichipi-Ifukor, Benneth Ben-Azu, Samuel Ogheneovo Asagba, Fidelis Ifeakachuku Achuba, John Chukwuma Oyem
BioMetals.2024; 37(2): 477. CrossRef - Surgical outcome after thyroidectomy due to Graves’ disease and Lugol iodine treatment: a retrospective register-based cohort study
Fredric Hedberg, Henrik Falhammar, Jan Calissendorff, Robert Bränström
Endocrine.2024;[Epub] CrossRef - Graves disease is associated with increased risk of clinical Alzheimer’s disease: evidence from the Medicare system
Arseniy Pavlovich Yashkin, Stanislav Kolpakov, Svetlana Ukraintseva, Anatoliy Yashin, Igor Akushevich
Clinical Diabetes and Endocrinology.2024;[Epub] CrossRef - A 2023 International Survey of Clinical Practice Patterns in the Management of Graves Disease: A Decade of Change
Danilo Villagelin, David S Cooper, Henry B Burch
The Journal of Clinical Endocrinology & Metabolism.2024;[Epub] CrossRef - Predictors of Prolonged Euthyroidism After Radioactive Iodine Treatment for Graves’ Disease: A Pilot Study
Jin-Ying Lu, Kuan-Hua Chen, Shyang-Rong Shih, Fang-Yu Wen, Wan-Chen Wu, Ting-Chu Chen, Fu-Chang Hu
Endocrine Practice.2023; 29(2): 89. CrossRef - Case of Graves’ disease recovery
Andrey Valerievich Ushakov
Journal of Clinical and Translational Endocrinology: Case Reports.2023; 27: 100139. CrossRef - Outcomes of Radioactive Iodine Versus Surgery for the Treatment of Graves’ Disease: a Systematic Review and Meta-analysis
Mohamed AbdAlla Salman, Mohamed Moustafa Assal, Ahmed Salman, Mohammed Elsherbiney
Indian Journal of Surgery.2023;[Epub] CrossRef - Association between high mobility group box-1 circulation level and Graves' ophthalmopathy
Mohammad Robikhul Ikhsan, Nyoman Kertia, Supanji Supanji, Bambang Udji djoko Rianto, Dhite Bayu Nugroho
F1000Research.2023; 12: 767. CrossRef - New-onset and relapsed Graves’ disease following COVID-19 vaccination: a comprehensive review of reported cases
Kan Chen, Yiyang Gao, Jing Li
European Journal of Medical Research.2023;[Epub] CrossRef - REVIEW OF SARS-CORONAVIRUS-2 REPERCUSSIONS ON THYROID GLAND IN THE CONTEXT OF HYPERTHYROIDISM
SHUBHAM SINGH, MONIKA, RUPA MAZUMDER, AVIJIT MAZUMDER
International Journal of Applied Pharmaceutics.2023; : 17. CrossRef - Effectiveness and potential mechanism of Jiawei-Xiaoyao-San for hyperthyroidism: a systematic review
Wenxin Ma, Xiaowen Zhang, Ruotong Zhao, Yang Tang, Xiaoyun Zhu, Longkun Liu, Mingyuan Xu, Ge Wang, Peiyue Peng, Jianping Liu, Zhaolan Liu
Frontiers in Endocrinology.2023;[Epub] CrossRef - Associations of serum keratin 1 with thyroid function and immunity in Graves’ disease
Chao-Wen Cheng, Wen-Fang Fang, Jiunn-Diann Lin, Appuwawadu Mestri Nipun Lakshitha de Silva
PLOS ONE.2023; 18(11): e0289345. CrossRef - Management of Graves’ hyperthyroidism: present and future
Luigi Bartalena, Eliana Piantanida, Daniela Gallo, Silvia Ippolito, Maria Laura Tanda
Expert Review of Endocrinology & Metabolism.2022; 17(2): 153. CrossRef - The Prediction Model Using Thyroid-stimulating Immunoglobulin Bioassay For Relapse of Graves’ Disease
Han-Sang Baek, Jaejun Lee, Chai-Ho Jeong, Jeongmin Lee, Jeonghoon Ha, Kwanhoon Jo, Min-Hee Kim, Jae Hyoung Cho, Moo Il Kang, Dong-Jun Lim
Journal of the Endocrine Society.2022;[Epub] CrossRef - Efficacy of Radioiodine Therapy in Patients With Primary Hyperthyroidism: An Institutional Review From Pakistan
Asim Munir Alvi, Umal Azmat, Waqas Shafiq, Abdul Hannan Ali Rasheed, Ahmed Imran Siddiqi, Sardar Khan, Sara Ashfaq, Hira Irfan , Humayun Bashir, Muhammad Abu Bakar, Kashif Asghar
Cureus.2022;[Epub] CrossRef - Clinical Outcomes of Repeated Radioactive Iodine Therapy for Graves’ Disease
Min Joo Kim, Sun Wook Cho, Ye An Kim, Hoon Sung Choi, Young Joo Park, Do Joon Park, Bo Youn Cho
Endocrinology and Metabolism.2022; 37(3): 524. CrossRef - Endocrine Surgery and Pediatic Surgery Partnership Reduces Complication Rate of Pediatric Thyroidectomy
Ali Sayan, Mehmet Üstün, Mehmet Mert, Cem Karaali, Gökhan Köylüoğlu
Journal of Dr Behcet Uz Children s Hospital.2022; 12(2): 164. CrossRef - Thyroid-related adverse events induced by immune checkpoint inhibitors
Alexandra Chera, Andreea Lucia Stancu, Octavian Bucur
Frontiers in Endocrinology.2022;[Epub] CrossRef - A case of Hashimoto's thyroiditis following Graves' disease
Ibtissem Oueslati, Salma Salhi, Meriem Yazidi, Fatma Chaker, Melika Chihaoui
Clinical Case Reports.2022;[Epub] CrossRef - Changes in the T and B lymphocyte subset profiles upon treatment of patients with Graves’ disease with radioactive iodine
A. A. Savchenko, M. A. Dudina, S. A. Dogadin, A. G. Borisov, I. V. Kudryavtsev, D. V. Fomina, V. D. Belenyuk
Medical Immunology (Russia).2022; 24(5): 1007. CrossRef - A survey of the young person’s experience of Graves’ disease and its management
Laura Claire Lane, Judith Rankin, Tim Cheetham
Clinical Endocrinology.2021; 94(2): 330. CrossRef - Serum T3 Level and Duration of Minimum Maintenance Dose Therapy Predict Relapse in Methimazole-Treated Graves Disease
Yotsapon Thewjitcharoen, Krittadhee Karndumri, Waralee Chatchomchuan, Sriurai Porramatikul, Sirinate Krittiyawong, Ekgaluck Wanothayaroj, Siriwan Butadej, Soontaree Nakasatien, Rajata Rajatanavin, Thep Himathongkam
Journal of the Endocrine Society.2021;[Epub] CrossRef - Dosimetry-guided radioiodine therapy of hyperthyroidism: long-term experience and implications for guidelines
Thomas Leitha, Manuela Schartel, Ingrid Hurtl, Rudolf Bednar, Franz König, Karl Mayrhofer, Flavia Pietschmann
Nuclear Medicine Communications.2021; 42(2): 150. CrossRef - Practice patterns and outcomes in the management of Thai patients with Graves’ disease
Yotsapon Thewjitcharoen, Krittadhee Karndumri, Waralee Chatchomchuan, Sriurai Porramatikul, Sirinate Krittiyawong, Ekgaluck Wanathayanoroj, Nampetch Lekpittaya, Worawit Kittipoom, Tawee Anuntakulnatee, Somboon Vongterapak, Siriwan Butadej, Soontaree Nakas
Thyroid Research.2021;[Epub] CrossRef - Un case report letterario di tireotossicosi in La coscienza di Zeno di Italo Svevo
Francesco Trimarchi, Luigi Bartalena, Stefano Arieti, Roberto Toni
L'Endocrinologo.2021; 22(2): 149. CrossRef - Medical treatment of thyrotoxicosis
Lorenzo SCAPPATICCIO, Giuseppe BELLASTELLA, Maria I. MAIORINO, Luca GIOVANELLA, Katherine ESPOSITO
The Quarterly Journal of Nuclear Medicine and Molecular Imaging.2021;[Epub] CrossRef - Hiccups as a Rare Presentation of Thyrotoxicosis Triaged by an Epidural Steroid Injection
Omar Al-Radideh, Iyad Farouji, Theodore DaCosta, Hossam Abed, Nicholas Baranestky
Cureus.2021;[Epub] CrossRef - Long-term antithyroid drug therapy
David S. Cooper
Current Opinion in Endocrinology, Diabetes & Obesity.2021; 28(5): 510. CrossRef - The Continuum of Thyroid Disorders Related to Immune Checkpoint Inhibitors: Still Many Pending Queries
Maria V. Deligiorgi, Sofia Sagredou, Lampros Vakkas, Dimitrios T. Trafalis
Cancers.2021; 13(21): 5277. CrossRef - Recurrence of Graves’ Disease: What Genetics of HLA and PTPN22 Can Tell Us
Daniela Vejrazkova, Josef Vcelak, Eliska Vaclavikova, Marketa Vankova, Katerina Zajickova, Jana Vrbikova, Michaela Duskova, Petra Pacesova, Zdenek Novak, Bela Bendlova
Frontiers in Endocrinology.2021;[Epub] CrossRef - Most Patients with Graves’ Disease Treated with Antithyroid Drugs Eventually Require Additional Therapies
Mary H. Samuels
Clinical Thyroidology.2020; 32(1): 9. CrossRef - Patterns of Use, Efficacy, and Safety of Treatment Options for Patients with Graves' Disease: A Nationwide Population-Based Study
Juan P. Brito, Stephanie Payne, Naykky Singh Ospina, Rene Rodriguez-Gutierrez, Spyridoula Maraka, Lindsey R. Sangaralingham, Nicole M. Iñiguez-Ariza, Victor M. Montori, Marius N. Stan
Thyroid.2020; 30(3): 357. CrossRef - Long-Term Treatment of Hyperthyroidism with Antithyroid Drugs: 35 Years of Personal Clinical Experience
Fereidoun Azizi
Thyroid.2020; 30(10): 1451. CrossRef - Predictive factors for early hypothyroidism following the radioactive iodine therapy in Graves’ disease patients
Rui-Ting Hu, De-Shan Liu, Bin Li
BMC Endocrine Disorders.2020;[Epub] CrossRef - The Concept of Cure in Thyroid Diseases
Fereidoun Azizi
International Journal of Endocrinology and Metabolism.2020;[Epub] CrossRef - Der Biomarker TSH bei Schilddrüsenautonomien
K. Passek, N. Zulauf, E. Wanke, G. M. Oremek
Zentralblatt für Arbeitsmedizin, Arbeitsschutz und Ergonomie.2020; 70(4): 177. CrossRef - Management of Graves’ Hyperthyroidism: More Than a Century of Progression
Hengameh Abdi, Atieh Amouzegar
International Journal of Endocrinology and Metabolism.2020;[Epub] CrossRef - Corticosteroid Pulse Therapy for Graves' Ophthalmopathy Reduces the Relapse Rate of Graves' Hyperthyroidism
Rosario Le Moli, Pasqualino Malandrino, Marco Russo, Fabrizio Lo Giudice, Francesco Frasca, Antonino Belfiore, Riccardo Vigneri
Frontiers in Endocrinology.2020;[Epub] CrossRef - Prediction of Relapse After Antithyroid Drugs Withdrawal: A Narrative Review
Pei-Wen Wang
International Journal of Endocrinology and Metabolism.2020;[Epub] CrossRef - Radioiodine-131 therapy (RIT) in benign thyroid diseases: Personalized prescription based on objectives with optional use of pharmacological modulators
J. Clerc
Médecine Nucléaire.2020; 44(4): 250. CrossRef - Predicting the Risk of Graves Disease Relapse: Commentary on “Thyroid Peroxidase Antibody Positivity is Associated with Relapse-Free Survival Following Antithyroid Drug Treatment for Graves Disease”
D. Gallo, M.L. Tanda, E. Piantanida
Endocrine Practice.2020; 26(9): 1039. CrossRef - Integrating Five Feature Types Extracted From Ultrasonograms to Improve the Prediction of Thyroid Papillary Carcinoma
Renxiang Zhu, Zhongyu Wang, Yifan Zhang, Bingxin Yu, Mingran Qi, Xin Feng, Chenjun Wu, Yuxuan Cui, Lan Huang, Fan Li, Fengfeng Zhou
IEEE Access.2019; 7: 101820. CrossRef - Serum TSH Receptor Antibodies Fall Gradually and Only Rarely Switch Functional Activity in Treated Graves’ Disease
Mary H. Samuels
Clinical Thyroidology.2019; 31(8): 330. CrossRef - Changes in Thyroid Peroxidase and Thyroglobulin Antibodies Might Be Associated with Graves' Disease Relapse after Antithyroid Drug Therapy
Yun Mi Choi, Mi Kyung Kwak, Sang Mo Hong, Eun-Gyoung Hong
Endocrinology and Metabolism.2019; 34(3): 268. CrossRef - A transgenic mouse that spontaneously develops pathogenic TSH receptor antibodies will facilitate study of antigen-specific immunotherapy for human Graves’ disease
Sandra M. McLachlan, Basil Rapoport
Endocrine.2019; 66(2): 137. CrossRef
- Multifunctional nanoparticle-mediated combining therapy for human diseases
- Thyroid
- Clinical Relevance of Environmental Factors in the Pathogenesis of Autoimmune Thyroid Disease
- Wilmar M. Wiersinga
- Endocrinol Metab. 2016;31(2):213-222. Published online May 13, 2016
- DOI: https://doi.org/10.3803/EnM.2016.31.2.213
- 9,201 View
- 212 Download
- 89 Web of Science
- 93 Crossref
-
Abstract
PDFPubReader
Genetic factors contribute for about 70% to 80% and environmental factors for about 20% to 30% to the pathogenesis of autoimmune thyroid disease (AITD). Relatives of AITD patients carry a risk to contract AITD themselves. The 5-year risk can be quantified by the so-called Thyroid Events Amsterdam-score, based on serum thyroid-stimulating hormone, thyroid peroxidase (TPO)-antibodies and family history. Subjects at risk may ask what they can do to prevent development of AITD. This review summarizes what is known about modulation of exposure to environmental factors in terms of AITD prevention. To stop smoking decreases the risk on Graves disease but increases the risk on Hashimoto disease. Moderate alcohol intake provides some protection against both Graves and Hashimoto disease. Low selenium intake is associated with a higher prevalence of thyroid autoimmunity, but evidence that selenium supplementation may lower TPO antibodies and prevent subclinical hypothyroidism remains inconclusive. Low serum vitamin D levels are associated with a higher prevalence of TPO antibodies, but intervention studies with extra vitamin D have not been done yet. Stress may provoke Graves hyperthyroidism but not Hashimoto thyroiditis. Estrogen use have been linked to a lower prevalence of Graves disease. The postpartum period is associated with an increased risk of AITD. Taking together, preventive interventions to diminish the risk of AITD are few, not always feasible, and probably of limited efficacy.
-
Citations
Citations to this article as recorded by- Trends in Prevalence of Thyroid Dysfunction and its Associations With Mortality Among US Participants, 1988-2012
Xiaowen Zhang, Yong Wang, Hongwei Wang, Xinlin Zhang
The Journal of Clinical Endocrinology & Metabolism.2024; 109(2): e657. CrossRef - The role of medical and organizational measures in improving the quality of early detection and clinical examination of autoimmune thyroiditis among the population of the Republic of Belarus
L. I. Danilova, V. A. Rozhko, I. V. Veyalkin, S. N. Nikanovich, T. M. Sharshakova
Health and Ecology Issues.2024; 20(4): 129. CrossRef - Hyperthyroidism
Layal Chaker, David S Cooper, John P Walsh, Robin P Peeters
The Lancet.2024; 403(10428): 768. CrossRef - A Review of Thyroid Dysfunction Due to COVID-19
Alireza Arefzadeh
Mini-Reviews in Medicinal Chemistry.2024; 24(3): 265. CrossRef - Alteration in kynurenine pathway metabolites in young women with autoimmune thyroiditis
Anna Krupa, Agnieszka Łebkowska, Marcin Kondraciuk, Karol Adam Kaminski, Irina Kowalska
Scientific Reports.2024;[Epub] CrossRef - Association of autoimmune thyroid disease with type 1 diabetes mellitus and its ultrasonic diagnosis and management
Jin Wang, Ke Wan, Xin Chang, Rui-Feng Mao
World Journal of Diabetes.2024; 15(3): 348. CrossRef - Hashimoto’s thyroiditis and coexisting disorders in correlation with HLA status—an overview
Peter Mikosch, Adrian Aistleitner, Markus Oehrlein, Eva Trifina-Mikosch
Wiener Medizinische Wochenschrift.2023; 173(1-2): 41. CrossRef - The management and metabolic characterization: hyperthyroidism and hypothyroidism
Yangyang Wang, YanPing Sun, Bingyou Yang, Qiuhong Wang, Haixue Kuang
Neuropeptides.2023; 97: 102308. CrossRef - Zn and Se abrogate heavy metal mixture induced ovarian and thyroid oxido-inflammatory effects mediated by activation of NRF2-HMOX-1 in female albino rats
Boma F. Eddie-Amadi, Anthonet N. Ezejiofor, Chinna N. Orish, Orish E. Orisakwe
Current Research in Toxicology.2023; 4: 100098. CrossRef - Genetically predicted selenium concentrations and thyroid function: A two‐sample Mendelian randomization study
Hui‐Jun Huang, Shan‐Shan Wang, Ming‐Min Jin, Bin‐Wei Cheng, Yu Liu, Xiao‐Chen Liu, Qiu‐Yan Yu, Xin‐Jun Yang
Clinical Endocrinology.2023; 98(6): 813. CrossRef - Identification of Smoking-Associated Transcriptome Aberration in Blood with Machine Learning Methods
FeiMing Huang, QingLan Ma, JingXin Ren, JiaRui Li, Fen Wang, Tao Huang, Yu-Dong Cai, Bilal Alatas
BioMed Research International.2023; 2023: 1. CrossRef - COVID-induced thyroid autoimmunity
Alessandro Brancatella, Nicola Viola, Ferruccio Santini, Francesco Latrofa
Best Practice & Research Clinical Endocrinology & Metabolism.2023; 37(2): 101742. CrossRef - Associations between vitamin D levels and dietary patterns in patients with Hashimoto’s thyroiditis
Dean Kaličanin, Maja Cvek, Ana Barić, Veselin Škrabić, Ante Punda, Vesna Boraska Perica
Frontiers in Nutrition.2023;[Epub] CrossRef - COMPARATIVE MORPHOLOGY OF THE THYROID GLAND
L. O. Sviatotska
Bulletin of Problems Biology and Medicine.2023; 1(2): 386. CrossRef - Evaluation and epigenetic impact of B12, vitamin D, folic acid and anemia in Hashimoto's thyroiditis: a clinical and molecular docking study
Elif Sibel ASLAN, Savaş GÜR
Journal of Health Sciences and Medicine.2023; 6(4): 705. CrossRef - Interactions between Polygenetic Variants and Lifestyle Factors in Hypothyroidism: A Hospital-Based Cohort Study
Da Sol Kim, Sunmin Park
Nutrients.2023; 15(17): 3850. CrossRef - Do Dietary Supplements Affect Inflammation, Oxidative Stress, and Antioxidant Status in Adults with Hypothyroidism or Hashimoto’s Disease?—A Systematic Review of Controlled Trials
Katarzyna Kubiak, Maria Karolina Szmidt, Joanna Kaluza, Agnieszka Zylka, Ewa Sicinska
Antioxidants.2023; 12(10): 1798. CrossRef - Identification and Preliminary Clinical Validation of Key Extracellular Proteins as the Potential Biomarkers in Hashimoto’s Thyroiditis by Comprehensive Analysis
Zihan Xi, Tinglin Yang, Tao Huang, Jun Zhou, Peng Yang
Biomedicines.2023; 11(12): 3127. CrossRef - An examination of retinal findings with optical coherence tomography in hypothyroidism patients with vitamin D deficiency: A comparative study
Samet Sayılan, Dila Kırağı, Mehmet Tayfun Arslan
Journal of Clinical Medicine of Kazakhstan.2023; 20(6): 36. CrossRef - The role of IL-4 −590 (C>T) Gene as diagnostic biomarker of Hashimoto thyroiditis disease patients in AL-Najaf provenance /Iraq
Sarah Hasan Kadhum AL-Huchaimi, Mahdi Hussain AL-Ammar, Sabah N. AL-Fatlawi
Al-Kufa University Journal for Biology.2023; 15(3): 14. CrossRef - Early life stress in women with autoimmune thyroid disorders
Alessia Corso, Hermann Engel, Fabienne Müller, Serena Fiacco, Laura Mernone, Elena Gardini, Ulrike Ehlert, Susanne Fischer
Scientific Reports.2023;[Epub] CrossRef - Protective Effects of Selenium and Zinc Against Nickel Chloride–Induced Hormonal Changes and Oxidative Damage in Thyroid of Pregnant Rats
Imane Salah, Ounassa Adjroud, Awatef Elwej
Biological Trace Element Research.2022; 200(5): 2183. CrossRef - Effects of animal protein intake during pregnancy on autoimmune thyroiditis in pregnant women with mild iodine deficiency
Zhengyuan Wang, Jiaying Shen, Qi Song, Xueying Cui, Zehuan Shi, Jin Su, Jiajie Zang
Journal of Human Nutrition and Dietetics.2022; 35(3): 542. CrossRef - Positive antithyroid antibody predicts severity of neuromyelitis optica spectrum disorder in children
Liang Huo, Hua Wang, Yujun Yuan, Jian Gao, Xueyan Liu
Multiple Sclerosis and Related Disorders.2022; 57: 103425. CrossRef - Seasonality of month of birth in patients with autoimmune endocrine diseases: A systematic review
Ana M. Ramos-Leví, Gloria Collado, Monica Marazuela
Endocrinología, Diabetes y Nutrición.2022; 69(10): 779. CrossRef - Are ethnic differences, urinary iodine status, lead and cadmium exposure associated with thyroid autoimmunity and hypothyroid status? A cross-sectional study
Yi Chen, Qian Xiang, Ningjian Wang, Wen Zhang, Chunfang Zhu, Yuying Wang, Heng Wan, Jing Cheng, Kun Zhang, Yan Cai, Yingli Lu
BMJ Open.2022; 12(2): e056909. CrossRef - The Association of Thyroid Nodules With Blood Trace Elements Identified in a Cross-Section Study
Huixian Zeng, Yuanyuan Hu, Yaosheng Luo, Yanshi Ye, Cheng Song, Genfeng Yu, Zhi Chen, Siyang Liu, Yongqian Liang, Lingling Liu, Heng Wan, Jie Shen
Frontiers in Nutrition.2022;[Epub] CrossRef - Nutritional Management of Thyroiditis of Hashimoto
Yana Danailova, Tsvetelina Velikova, Georgi Nikolaev, Zorka Mitova, Alexander Shinkov, Hristo Gagov, Rossitza Konakchieva
International Journal of Molecular Sciences.2022; 23(9): 5144. CrossRef - Association Between Vitamin D Deficiency and Autoimmune Thyroid Disorder: A Systematic Review
Sabah A Khozam, Abdulhadi M Sumaili, Mohammed A Alflan, Rawan As'ad Salameh Shawabkeh
Cureus.2022;[Epub] CrossRef - Metabolic Characteristics of Hashimoto’s Thyroiditis Patients and the Role of Microelements and Diet in the Disease Management—An Overview
Aniceta A. Mikulska, Marta Karaźniewicz-Łada, Dorota Filipowicz, Marek Ruchała, Franciszek K. Główka
International Journal of Molecular Sciences.2022; 23(12): 6580. CrossRef - Predictors of autoimmune thyroid disease
Carol Cardona Attard, W. C. Candy Sze, Sandro Vella
Baylor University Medical Center Proceedings.2022; 35(5): 608. CrossRef - Selenium Status and Supplementation Effects in Pregnancy—A Study on Mother–Child Pairs from a Single-Center Cohort
Dorota Filipowicz, Ewelina Szczepanek-Parulska, Małgorzata Kłobus, Krzysztof Szymanowski, Thilo Samson Chillon, Sabrina Asaad, Qian Sun, Aniceta A. Mikulska-Sauermann, Marta Karaźniewicz-Łada, Franciszek K. Główka, Dominika Wietrzyk, Lutz Schomburg, Marek
Nutrients.2022; 14(15): 3082. CrossRef - Inflammasome activation as a link between obesity and thyroid disorders: Implications for an integrated clinical management
Rosario Le Moli, Veronica Vella, Dario Tumino, Tommaso Piticchio, Adriano Naselli, Antonino Belfiore, Francesco Frasca
Frontiers in Endocrinology.2022;[Epub] CrossRef - Seasonality of month of birth in patients with autoimmune endocrine diseases: A systematic review
Ana M. Ramos-Leví, Gloria Collado, Monica Marazuela
Endocrinología, Diabetes y Nutrición (English ed.).2022; 69(10): 779. CrossRef - Impact of iodine intake on the pathogenesis of autoimmune thyroid disease in children and adults
Iyshwarya Bhaskar Kalarani, Ramakrishnan Veerabathiran
Annals of Pediatric Endocrinology & Metabolism.2022; 27(4): 256. CrossRef - Morphological features of thyroid benign focal neoplasms in Graves’ disease
Yu.V. Buldygina, A.V. Zelinskaya, L.Yu. Zurnadzhy, Yu.M. Tarashchenko, S.L. Shlyakhtych, M.D. Tronko
INTERNATIONAL JOURNAL OF ENDOCRINOLOGY (Ukraine).2022; 18(4): 213. CrossRef - Onset of Marine-Lenhart syndrome and Graves’ ophthalmopathy in a female patient treated with alemtuzumab for multiple sclerosis
Rosario Le Moli, Marco Russo, Pasqualino Malandrino, Veronica Vella, Antonino Belfiore, Francesco Frasca
Hormones.2021; 20(1): 161. CrossRef - Limited Genetic Overlap Between Overt Hashimoto’s Thyroiditis and Graves’ Disease in Twins: A Population-based Study
Jakob Skov, Jan Calissendorff, Daniel Eriksson, Patrik Magnusson, Olle Kämpe, Sophie Bensing, Ralf Kuja-Halkola
The Journal of Clinical Endocrinology & Metabolism.2021; 106(4): e1101. CrossRef - DNA Methylation Patterns in the HLA-DPB1 and PDCD1LG2 Gene Regions in Patients with Autoimmune Thyroiditis from Different Water Iodine Areas
Siyuan Wan, Lixiang Liu, Bingxuan Ren, Mengying Qu, Huaiyong Wu, Wen Jiang, Xiaoming Wang, Hongmei Shen
Thyroid.2021; 31(11): 1741. CrossRef - Персоналізація лікування хвороби Грейвса на підставі клініко- імунологічних характеристик перебігу захворювання
Yu.V. Buldygina, S.L. Shlyakhtych, H.M. Terekhova, T.V. Fed’ko, V.M. Klochkova, L.S. Strafun, Z.H. Lysova, I.I. Savos’ko
Endokrynologia.2021; 26(4): 409. CrossRef - Parity and Incidence of Thyroid Autoimmunity: A Population-Based Tehran Thyroid Study
Miralireza Takyar, Maryam Rahmani, Atieh Amouzegar, Elham Madreseh, Maryam Tohidi, Ladan Mehran, Fereidoun Azizi
Thyroid.2020; 30(8): 1186. CrossRef - Immunomodulatory effect of vitamin D and its potential role in the prevention and treatment of thyroid autoimmunity: a narrative review
D. Gallo, L. Mortara, M. B. Gariboldi, S. A. M. Cattaneo, S. Rosetti, L. Gentile, D. M. Noonan, P. Premoli, C. Cusini, M. L. Tanda, L. Bartalena, E. Piantanida
Journal of Endocrinological Investigation.2020; 43(4): 413. CrossRef - Hashimoto Thyreoiditis, therapeutische Optionen und extrathyreoidale Assoziationen – ein aktueller Überblick
Eva Petnehazy, Wolfgang Buchinger
Wiener Medizinische Wochenschrift.2020; 170(1-2): 26. CrossRef - Pathophysiological Role and Therapeutic Implications of Vitamin D in Autoimmunity: Focus on Chronic Autoimmune Diseases
Mattia Bellan, Laura Andreoli, Chiara Mele, Pier Paolo Sainaghi, Cristina Rigamonti, Silvia Piantoni, Carla De Benedittis, Gianluca Aimaretti, Mario Pirisi, Paolo Marzullo
Nutrients.2020; 12(3): 789. CrossRef - Thyroxine-binding globulin, peripheral deiodinase activity, and thyroid autoantibody status in association of phthalates and phenolic compounds with thyroid hormones in adult population
Sohyeon Choi, Min Joo Kim, Young Joo Park, Sunmi Kim, Kyungho Choi, Gi Jeong Cheon, Yoon Hee Cho, Hye Li Jeon, Jiyoung Yoo, Jeongim Park
Environment International.2020; 140: 105783. CrossRef - Immunomodulatory Effects of Vitamin D in Thyroid Diseases
Chiara Mele, Marina Caputo, Alessandro Bisceglia, Maria Teresa Samà, Marco Zavattaro, Gianluca Aimaretti, Loredana Pagano, Flavia Prodam, Paolo Marzullo
Nutrients.2020; 12(5): 1444. CrossRef - Significance of arsenic and lead in Hashimoto's thyroiditis demonstrated on thyroid tissue, blood, and urine samples
Aleksandar Stojsavljević, Branislav Rovčanin, Jovana Jagodić, Danijela Drašković Radojković, Ivan Paunović, Marija Gavrović-Jankulović, Dragan Manojlović
Environmental Research.2020; 186: 109538. CrossRef - Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses
Alessandro Antonelli, Silvia Martina Ferrari, Francesca Ragusa, Giusy Elia, Sabrina Rosaria Paparo, Ilaria Ruffilli, Armando Patrizio, Claudia Giusti, Debora Gonnella, Alfonso Cristaudo, Rudy Foddis, Yehuda Shoenfeld, Poupak Fallahi
Best Practice & Research Clinical Endocrinology & Metabolism.2020; 34(1): 101387. CrossRef - Vitamin D deficiency and thyroid autoantibody fluctuations in patients with Graves’ disease – A mere coincidence or a real relationship?
Maria Teresa Płazińska, Agata Czarnywojtek, Nadia Sawicka-Gutaj, Małgorzata Zgorzalewicz-Stachowiak, Barbara Czarnocka, Paweł Gut, Maria Karlinska, Marta Fichna, Adam Stachowski, Marek Ruchała, Iwona Krela-Kaźmierczak, Leszek Królicki
Advances in Medical Sciences.2020; 65(1): 39. CrossRef - An eight-year-old girl with autoimmune polyglandular syndrome type3A that developed during the course of primary Epstein–Barr virus (EBV) infection: clinical implication of EBV in autoimmune thyroid disease
Shizuka Kirino, Hisae Nakatani, Aoi Honma, Asami Shinbo, Keiko Onda, Mari Okada, Masako Imai, Natsuko Suzuki, Akihiro Oshiba, Masayuki Nagasawa
Immunological Medicine.2020; 43(1): 57. CrossRef - Exploring the role of copper and selenium in the maintenance of normal thyroid function among healthy Koreans
Min Joo Kim, Soo Chin Kim, Soie Chung, Serim Kim, Ji Won Yoon, Young Joo Park
Journal of Trace Elements in Medicine and Biology.2020; 61: 126558. CrossRef - A comparison of serum zinc levels in melasma and non-melasma patients: a preliminary study of thyroid dysfunction
Indina Sastrini Sekarnesia, Irma Bernadette S. Sitohang, Triana Agustin, Wismandari Wisnu, Aida S. D. Hoemardani
Acta Dermatovenerologica Alpina Pannonica et Adriatica.2020;[Epub] CrossRef - Hashimoto's thyroiditis: An update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential malignant transformation
Massimo Ralli, Diletta Angeletti, Marco Fiore, Vittorio D'Aguanno, Alessandro Lambiase, Marco Artico, Marco de Vincentiis, Antonio Greco
Autoimmunity Reviews.2020; 19(10): 102649. CrossRef - Vitamin D and Autoimmune Thyroid Disease—Cause, Consequence, or a Vicious Cycle?
Inês Henriques Vieira, Dírcea Rodrigues, Isabel Paiva
Nutrients.2020; 12(9): 2791. CrossRef - New Insights into Mechanisms of Endocrine-Disrupting Chemicals in Thyroid Diseases: The Epigenetic Way
Letizia Pitto, Francesca Gorini, Fabrizio Bianchi, Elena Guzzolino
International Journal of Environmental Research and Public Health.2020; 17(21): 7787. CrossRef - Genotype association of IP6K3 gene with Hashimoto’s thyroiditis in Algerian population (Aures region)
Warda Kherrour, Dean Kalicanin, Luka Brčić, Leila Hambaba, Mouloud Yahia, Souheyla Benbia, Vesna Boraska Perica
Egyptian Journal of Medical Human Genetics.2020;[Epub] CrossRef - TOTAL ANTIOXIDANT ACTIVITY AND MANGANESE SUPEROXIDE DISMUTASE IN COMORBIDITY OF GASTROESOPHAGEAL REFLUX DISEASE AND AUTOIMMUNE THYROIDITIS IN STUDENT POPULATION
Tamara M. Pasiieshvili, Natalia M. Zhelezniakova, Lyudmila M. Pasiyeshvili, Olga M. Kovalyova
Wiadomości Lekarskie.2020; 73(12): 2644. CrossRef - Vitamin B12 and Vitamin D Levels in Patients with Autoimmune Hypothyroidism and Their Correlation with Anti-Thyroid Peroxidase Antibodies
Hanife Şerife Aktaş
Medical Principles and Practice.2020; 29(4): 364. CrossRef - Increased Risk of Thyroid Dysfunction Among Patients With Rheumatoid Arthritis
Qian Li, Bin Wang, Kaida Mu, Jing Zhang, Yanping Yang, Wei Yao, Jie Zhu, Jin-an Zhang
Frontiers in Endocrinology.2019;[Epub] CrossRef - Association between thyroglobulin polymorphisms and autoimmune thyroid disease: a systematic review and meta-analysis of case–control studies
Ming-Liang Zhang, Dong-ming Zhang, Cai-E. Wang, Xiao-Long Chen, Fang-Zhou Liu, Jian-Xue Yang
Genes & Immunity.2019; 20(6): 484. CrossRef - Changes in glucose‐lipid metabolism, insulin resistance, and inflammatory factors in patients with autoimmune thyroid disease
Yi Lei, Jun Yang, Hua Li, Haihua Zhong, Qin Wan
Journal of Clinical Laboratory Analysis.2019;[Epub] CrossRef - Evaluation of Qualitative Dietary Protocol (Diet4Hashi) Application in Dietary Counseling in Hashimoto Thyroiditis: Study Protocol of a Randomized Controlled Trial
Natalia Wojtas, Lidia Wadolowska, Elżbieta Bandurska-Stankiewicz
International Journal of Environmental Research and Public Health.2019; 16(23): 4841. CrossRef - Sjögren’s Syndrome and Autoimmune Thyroid Disease: Two Sides of the Same Coin
Juan-Manuel Anaya, Paula Restrepo-Jiménez, Yhojan Rodríguez, Mónica Rodríguez-Jiménez, Yeny Acosta-Ampudia, Diana M. Monsalve, Yovana Pacheco, Carolina Ramírez-Santana, Nicolás Molano-González, Rubén D. Mantilla
Clinical Reviews in Allergy & Immunology.2019; 56(3): 362. CrossRef - Disease Presentation and Remission Rate in Graves Disease Treated With Antithyroid Drugs: is Gender Really A Factor?
Talia Diker-Cohen, Hadar Duskin-Bitan, Ilan Shimon, Dania Hirsch, Amit Akirov, Gloria Tsvetov, Eyal Robenshtok
Endocrine Practice.2019; 25(1): 43. CrossRef - IRAK2 and TLR10 confer risk of Hashimoto’s disease: a genetic association study based on the Han Chinese population
Miao Li, Wei Han, Li Zhu, Jue Jiang, Wei Qu, Lei Zhang, Liang Jia, Qi Zhou
Journal of Human Genetics.2019; 64(7): 617. CrossRef - Environmental exposure to pesticides and risk of thyroid diseases
Mar Requena, Antonia López-Villén, Antonio F. Hernández, Tesifón Parrón, Ángela Navarro, Raquel Alarcón
Toxicology Letters.2019; 315: 55. CrossRef - Determining the Level of Knowledge about Graves’ Disease: Single-Center Results
Hande Peynirci, Çiğdem Uzuntepe Aksu, Akif Doğan, Canan Ersoy
Ankara Medical Journal.2019;[Epub] CrossRef - Association between lifestyle and thyroid dysfunction: a cross-sectional epidemiologic study in the She ethnic minority group of Fujian Province in China
Yanling Huang, Liangchun Cai, Yuanyuan Zheng, Jinxing Pan, Liantao Li, Liyao Zong, Wei Lin, Jixing Liang, Huibin Huang, Junping Wen, Gang Chen
BMC Endocrine Disorders.2019;[Epub] CrossRef - Vitamin D Receptor Gene Polymorphisms and Autoimmune Thyroiditis: Are They Associated with Disease Occurrence and Its Features?
Adam Maciejewski, Michał J. Kowalczyk, Waldemar Herman, Adam Czyżyk, Marta Kowalska, Ryszard Żaba, Katarzyna Łącka
BioMed Research International.2019; 2019: 1. CrossRef - Diagnosis of Graves’ disease – laboratory tests and possible difficulties in interpretation
Agata Maria Kalicka
Diagnostyka Laboratoryjna.2019; 55(2): 121. CrossRef - The influence of single-nucleotide polymorphisms of interleukin-1β -511 and +3954 on the susceptibility to Hashimoto’s thyroiditis in Egyptian women: immune-endocrine interactions
Nearmeen M. Rashad, Manar H. Soliman, Mayada M. Mousa, Azza H. Abd El-Fatah
The Egyptian Journal of Internal Medicine.2019; 31(1): 14. CrossRef - Global epidemiology of hyperthyroidism and hypothyroidism
Peter N. Taylor, Diana Albrecht, Anna Scholz, Gala Gutierrez-Buey, John H. Lazarus, Colin M. Dayan, Onyebuchi E. Okosieme
Nature Reviews Endocrinology.2018; 14(5): 301. CrossRef - Selenoproteins in human body: focus on thyroid pathophysiology
Ana Valea, Carmen Emanuela Georgescu
Hormones.2018; 17(2): 183. CrossRef - Epidemiology of hyperthyroidism in Iran: a systematic review and meta-analysis
Sayed Mahmoud Sajjadi-Jazi, Farshad Sharifi, Mehdi Varmaghani, Hamidreza Aghaei Meybodi, Farshad Farzadfar, Bagher Larijani
Journal of Diabetes & Metabolic Disorders.2018; 17(2): 345. CrossRef - The effect of vitamin D supplementation on thyroid autoantibody levels in the treatment of autoimmune thyroiditis: a systematic review and a meta-analysis
Su Wang, Yaping Wu, Zhihua Zuo, Yijing Zhao, Kun Wang
Endocrine.2018; 59(3): 499. CrossRef - Thyroid disorders in alemtuzumab-treated multiple sclerosis patients: a Belgian consensus on diagnosis and management
Brigitte Decallonne, Emmanuel Bartholomé, Valérie Delvaux, Miguel D’haeseleer, Souraya El Sankari, Pierrette Seeldrayers, Bart Van Wijmeersch, Chantal Daumerie
Acta Neurologica Belgica.2018; 118(2): 153. CrossRef - Synergistic interactions of Angiotensin Converting Enzyme (ACE) gene and Apolipoprotein E (APOE) gene polymorphisms with T1DM susceptibility in south India
Padma-Malini Ravi, Rathika Chinniah, Ramgopal Sivanadham, Murali Vijayan, Dharmarajan Pannerselvam, S. Pushkala, Balakrishnan Karuppiah
Meta Gene.2018; 18: 39. CrossRef - The effect of obesity and dietary habits on oxidative stress in Hashimoto’s thyroiditis
Maria Giannakou, Katerina Saltiki, Emily Mantzou, Eleni Loukari, Georgios Philippou, Konstantinos Terzidis, Charalampos Stavrianos, Miltiades Kyprianou, Theodora Psaltopoulou, Kalliopi Karatzi, Maria Alevizaki
Endocrine Connections.2018; 7(9): 990. CrossRef - Interaction of HLA-DRB1* alleles and CTLA4 (+ 49 AG) gene polymorphism in Autoimmune Thyroid Disease
Sivanadham Ramgopal, Chinniah Rathika, Malini Ravi Padma, Vijayan Murali, Kannan Arun, Mohamed Nainar Kamaludeen, Karuppiah Balakrishnan
Gene.2018; 642: 430. CrossRef - New insights into the etiopathogenesis of Hashimoto's Thyroiditis: The role of genetics and epigenetics
Massimo Ralli, Armando De Virgilio, Marco Artico, Lucia Longo, Marco de Vincentiis, Antonio Greco
Autoimmunity Reviews.2018; 17(10): 1065. CrossRef - Comorbidity of autoimmune thyroid disorders and psychiatric disorders during the postpartum period: a Danish nationwide register-based cohort study
V. Bergink, V. J. M. Pop, P. R. Nielsen, E. Agerbo, T. Munk-Olsen, X. Liu
Psychological Medicine.2018; 48(8): 1291. CrossRef - Spontaneous conversion from Graves’ disease to Hashimoto’s thyroiditis: a case report
Muharrem Bayrak, Kenan Çadırcı, Emine Kartal Baykan, Ünsal Aydın, Ayşe Çarlıoğlu
Ortadoğu Tıp Dergisi.2018; 10(1): 81. CrossRef - Association of established hypothyroidism-associated genetic variants with Hashimoto’s thyroiditis
A. Barić, L. Brčić, S. Gračan, V. Torlak Lovrić, I. Gunjača, M. Šimunac, M. Brekalo, M. Boban, O. Polašek, M. Barbalić, T. Zemunik, A. Punda, V. Boraska Perica
Journal of Endocrinological Investigation.2017; 40(10): 1061. CrossRef - Immune Response of Laying Hens Exposed to 30 ppm Ammonia
for 25 Weeks
H. Chen, F.F. Yan, J.Y. Hu, Yanan Wu, C.M. Tucker, A.R. Green, H.W. Cheng
International Journal of Poultry Science.2017; 16(4): 139. CrossRef - Dietary Factors Associated with Plasma Thyroid Peroxidase and Thyroglobulin Antibodies
Antonela Matana, Vesela Torlak, Dubravka Brdar, Marijana Popović, Bernarda Lozić, Maja Barbalić, Vesna Boraska Perica, Ante Punda, Ozren Polašek, Caroline Hayward, Tatijana Zemunik
Nutrients.2017; 9(11): 1186. CrossRef - Articles inEndocrinology and Metabolismin 2016
Won-Young Lee
Endocrinology and Metabolism.2017; 32(1): 62. CrossRef - Does vitamin D play a role in autoimmune endocrine disorders? A proof of concept
Barbara Altieri, Giovanna Muscogiuri, Luigi Barrea, Chantal Mathieu, Carla V. Vallone, Luca Mascitelli, Giorgia Bizzaro, Vincenzo M. Altieri, Giacomo Tirabassi, Giancarlo Balercia, Silvia Savastano, Nicola Bizzaro, Cristina L. Ronchi, Annamaria Colao, Alf
Reviews in Endocrine and Metabolic Disorders.2017; 18(3): 335. CrossRef - A case‐control study of the association between ulcerative colitis and hyperthyroidism in an Asian population
Ming‐Chieh Tsai, Herng‐Ching Lin, Cha‐Ze Lee
Clinical Endocrinology.2017; 86(6): 825. CrossRef - Hashimoto's thyroiditis: relative recurrence risk ratio and implications for screening of first‐degree relatives
Nikita Bothra, Nalini Shah, Manjunath Goroshi, Swati Jadhav, Sheetal Padalkar, Hemangini Thakkar, Gurudayal Singh Toteja, Vyankatesh Shivane, Anurag Lila, Tushar Bandgar
Clinical Endocrinology.2017; 87(2): 201. CrossRef - Serum 25-OH vitamin D levels in systemic sclerosis: analysis of 140 patients and review of the literature
Dilia Giuggioli, M. Colaci, G. Cassone, P. Fallahi, F. Lumetti, A. Spinella, F. Campomori, A. Manfredi, C. U. Manzini, A. Antonelli, C. Ferri
Clinical Rheumatology.2017; 36(3): 583. CrossRef - Are Perinatal Events Risk Factors for Childhood Thyroid Autoimmunity?
Berglind Jonsdottir, Markus Lundgren, Sara Wallengren, Åke Lernmark, Ida Jönsson, Helena Elding Larsson
European Thyroid Journal.2017; 6(6): 298. CrossRef - Variants of Interleukin-22 Gene Confer Predisposition to Autoimmune Thyroid Disease
Rong-hua Song, Qian Li, Wen Wang, Qiu-ming Yao, Xiao-qing Shao, Jin-an Zhang
International Journal of Endocrinology.2017; 2017: 1. CrossRef - Environmental Issues in Thyroid Diseases
Silvia Martina Ferrari, Poupak Fallahi, Alessandro Antonelli, Salvatore Benvenga
Frontiers in Endocrinology.2017;[Epub] CrossRef
- Trends in Prevalence of Thyroid Dysfunction and its Associations With Mortality Among US Participants, 1988-2012
 First
First Prev
Prev


